
by Maurice K. Chung, RPh, MD
In my decades of practice, I have embraced the transformation from open surgery to laparoscopy and finally to every-smaller, less invasive laparoscopic approaches such as mini lap. As a pelvic pain specialist who performs many endometriosis and urogynecological procedures, I know how these surgical technologies can improve both outcomes and the overall patient experience.
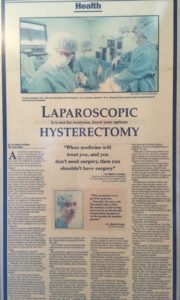
Advancing Laparoscopy
When I got my certification for laparoscopy in 1996, there were only about 100 of us in the first round of applicants. Within a few years, the number of physicians with that credential grew to about 1,000 in the U.S. Everyone else was performing vaginal and open surgery. Laparoscopy (using 10mm optics and a 10mm port site) was used primarily for tubal ligation and diagnosis.
Nevertheless, the advantages of this technology for our patients were clear from the start. Smaller incisions, less pain, and faster recovery made this an exciting modality to explore and continually improve. In time, gynecology moved on to using all 5mm instruments and port sizes, reducing our patients’ discomfort even further. Our list of laparoscopic procedures grew to include full and partial hysterectomy and fibroid removal.
In the early 2000s, the da Vinci System allowed more surgeons to capably perform laparoscopic procedures. However, in terms of cosmesis and pain, the robot is a bigger instrument with a 12mm umbilical port size for the camera and 10mm side ports for the assistant arms, so there is more scarring and pain than traditional laparoscopy. Though I selectively use the platform, I have also continued to work on enhancing traditional laparoscopy.
The Advent of Mini Lap
In 2010, new instrumentation allowed us to begin performing mini laparoscopy with sub-3mm incisions. At the start, we did not have radiofrequency energy or good suction, but a few of us began trying it for diagnosis. In time, energy devices improved and we gradually acquired better instrumentation for complex tasks. Now, more surgeons have begun adopting the procedure and I follow this approach for removal of the ovaries or uterus, excision of superficial or deep endometriosis, pelvic floor repair, and urinary incontinence procedures, among others.
For me, mini lap relies, in part, on advanced CO2 laser fiber technology. Our Lumenis UltraPulse Duo CO2 laser with FiberLase waveguide is precise, allowing me to cut a line with a 0.5mm spot size without thermal spread, reducing damage to adjacent tissue and minimizing complications. The laser is also powerful enough to allow me to quickly cut dense, fibrous tissue like butter. The fiber is perfect for small incisions.
For our patients, these technologies change the surgical experience. Of all the surgical options, mini lap disturbs tissue the least. Mini lap is slightly more difficult for the surgeon than standard laparoscopy (and easier for obese patients), so the duration of anesthesia is about the same. The small incisions, which do not even require a stitch, are cosmetically preferable. More importantly to our patients, there is less trauma and pain, which often allows me to discharge my patients within 2 hours. Patients undergoing hysterectomy still have a vaginal incision, but no abdominal trauma.
At some point, I think it will become possible to perform mini lap robotically. I’ll be the first to jump on it, and I am excited by the prospect of bringing mini lap to more patients, so they can have a better surgical experience.
Maurice K. Chung, RPh, MD, is Director at Mercy Regional Center of Excellence for Endometriosis, Pelvic Pain & Urogynecology in Canton, Ohio, and a Clinical Professor of Obstetrics/Gynecology at the University of Toledo School of Medicine.
The content presented on this page is provided for informational and/or educational purposes. This material represents the views and opinions of its authors and should not be construed as representing or reflecting the official position, views or opinions of the Society of Laparoendoscopic Surgeons. The authors of the work are solely responsible for its content.